Most modified duty programs fail because they are reactive. Here is the framework for building a proactive modified-duty library by role and restriction level, with templates for the HR, Safety, and Operations teams.
Almost every employer says they have a modified duty program. Far fewer actually have one. What most companies have is an intention: a line in the handbook that says light duty is available when appropriate, and a vague understanding that someone will figure it out when the time comes.
Then a worker gets hurt. The clinician sends back restrictions: no lifting over ten pounds, no overhead reaching, sit or stand as tolerated. And the scramble begins. A supervisor who has never thought about this before tries to invent a job on the spot. HR is not sure what is allowed. Operations does not want a body standing around who cannot do the real work. Days pass. The worker, still hurt and now sitting at home, starts to drift. And every day they sit at home, the claim gets more expensive and the odds of a clean return drop.
That is what a reactive modified-duty program looks like, and that is why so many of them quietly fail. The fix is not more willpower in the moment. It is doing the work before the injury, so that when restrictions come back, the answer already exists. This is how to build that proactive library, organized by role and by restriction level, with clear ownership across HR, Safety, and Operations. The templates are included.
Why reactive modified duty fails, and why it costs you so much
The case for getting this right is not subtle. Return-to-work research is some of the most consistent in the entire workers’ comp literature, and it all points in the same direction: time out of work is the enemy.
The American College of Occupational and Environmental Medicine has found that once an injured worker has been off the job for more than twelve weeks, the likelihood they will ever return to their original role drops to roughly 50%. After a full year out, it falls to about 5%. The worker does not usually fail to return because the injury was catastrophic. They fail to return because they got comfortable being out, lost their workplace identity and routine, and crossed a psychological line that gets harder to walk back every week.
Now look at what a real program does to the numbers. Insurers and researchers report that structured return-to-work programs reduce lost workdays due to occupational injuries by up to 55%. A frequently cited ten-year study published in the Journal of Occupational and Environmental Medicine tracked an employer’s program and found lost-time claims fell 73% and total workers’ comp costs fell 54% over the period, with lost-time claims paid per 100 employees dropping from 163 to 37. The RAND Institute for Civil Justice has documented that return-to-work programs cut missed time by several weeks per claim. And one analysis pegged the return at roughly $9 for every $1 spent standing the program up.
Against numbers like those, cutting lost-time claims by 40% is not an aggressive promise. It is a conservative, highly achievable target for an employer moving from reactive to proactive. The catch is the word proactive. The savings do not come from having a policy. They come from having the actual jobs identified, written down, and ready before anyone gets hurt.
The core idea: a library, not a scramble
A proactive modified-duty program is built around a simple asset: a library of transitional tasks, mapped to the restrictions they accommodate and the departments they apply to. Instead of inventing a light-duty assignment under pressure, the supervisor pulls from a shelf that is already stocked.
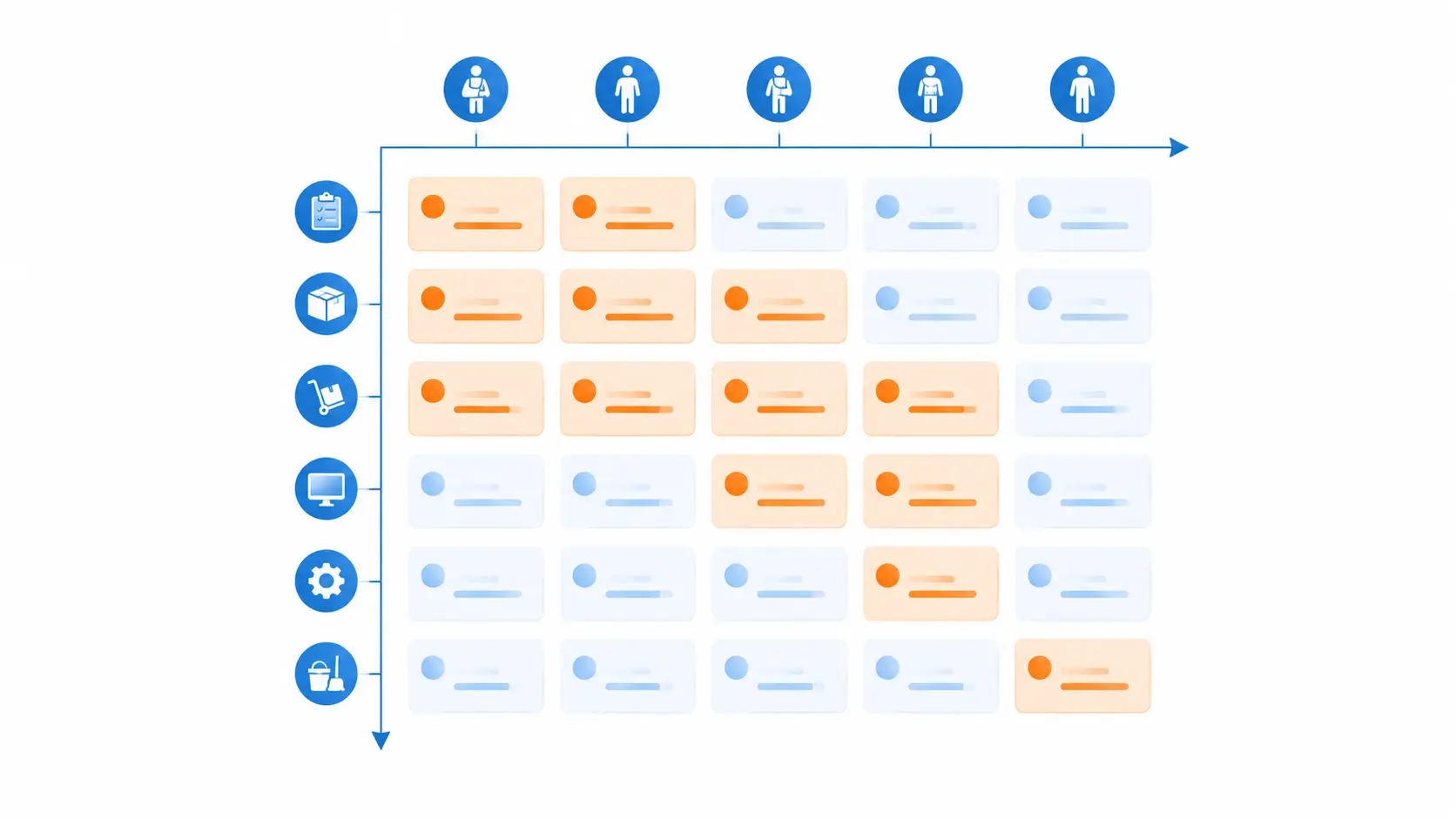
The library is organized along two axes.
The first axis is restriction level, because clinicians do not send back job titles; they send back physical limitations. If your library is organized by the restrictions that actually show up on clinical paperwork, you can match a worker to suitable tasks in minutes. The second axis is role and department, because a transitional task only works if it is real, supervised, and located where someone can actually oversee it. A meaningful task in the same department beats a made-up task in a corner every time.
Build the grid where those two axes meet, and you have something powerful: for any combination of restriction and department, a ready list of legitimate work the injured employee can do today.
The build, step by step
Step 1: Translate clinical restrictions into standard categories. Restrictions arrive in endless specific wordings, but they cluster into a manageable set of categories. Standardize them so the rest of the system has a common language. A workable starting menu:
- Lifting and carrying limits (for example, nothing over 10, 20, or 25 pounds)
- No overhead or limited overhead reaching
- No repetitive bending, twisting, or stooping
- Sit or stand as tolerated, with the ability to change position
- Limited standing or walking time per hour
- One-handed or one-arm duty
- No operation of heavy equipment or vehicles
- Limited hours or a graduated schedule
- No exposure to specific hazards (heat, vibration, certain chemicals)
Step 2: Run the “extra pair of hands” exercise with every department. This is the heart of the build, and it is the step most companies skip. Sit down with each operation and department leader and ask one question: if you had an extra, partially restricted person for a few weeks, what genuinely useful work would you hand them? You will be surprised how many surfaces: inventory cycle counts, quality audits, training new hires, documentation cleanup, tool and equipment checks, expediting, light assembly, monitoring and reporting, cross-training. The goal is real work that adds value, not busywork that signals to the worker that they are a burden.
Step 3: Score each task against the restriction categories. For every transitional task you collect, note the physical demands and which restriction categories it can safely accommodate. A cycle count might be fine for someone with a 10-pound limit and a sit-or-stand restriction, but unsuitable for someone who cannot stand for long. This scoring is what turns a list of ideas into a usable matching tool.
Step 4: Assign ownership before you need it. A program with no clear owner becomes everyone’s job, which means it is no one’s job. Decide in advance who maintains the library, who activates it when an injury occurs, who confirms the clinical restrictions, and who supervises the worker day-to-day. The clean split that works for most employers: Safety owns the task bank and keeps it current; HR owns compliance and the offer process; Operations owns supervision and day-to-day fit; and your clinical partner owns the restrictions themselves.
Step 5: Communicate the program before injuries happen. Tell workers at hire and at regular intervals that if they are ever hurt, the company has meaningful transitional work waiting and fully intends to keep them employed and earning. This single message defuses the fear that drives so many bad outcomes, the fear that an injury means lost income or a lost job. A worker who already knows the safety net exists behaves completely differently in the first hours after an injury.
Step 6: Build the activation workflow. When an injury occurs, the sequence should be automatic: immediate clinical contact and triage, documented restrictions, a match against the library, a written modified duty offer, and a start on transitional work, ideally without the worker ever losing a scheduled shift. The faster this runs, the more lost time you eliminate, because the indemnity clock and the psychological drift both start the moment the worker goes home.
Step 7: Measure the right things. Track lost-time claim frequency, the average lag from injury to first day of transitional duty, average days spent on transitional duty, and the rate of successful return to full duty. These four numbers tell you whether the library is actually being used and whether it is working.
The templates
Here are the starting templates the framework runs on. Copy them, adapt the categories to your operation, and fill them with your real tasks.
Template A: Transitional Task Bank. The master library. One row per task.
| Task | Department | Physical demands | Restriction categories it fits | Supervising owner |
|---|---|---|---|---|
| Inventory cycle counts | Warehouse | Light, sit or stand, occasional reach | 10 to 20 lb limit, sit/stand, one-handed | Warehouse lead |
| Quality audit and documentation | Production | Sedentary, mostly seated | Most restrictions, limited hours | QA supervisor |
| New-hire training and shadowing | Any | Light, verbal, mobile | No-lift, graduated schedule | Department lead |
| Tool and equipment inspection | Maintenance | Light, one-handed feasible | One-arm duty, no overhead | Maintenance lead |
Template B: Restriction Category Menu. The standardized list from Step 1 was posted so that clinicians, supervisors, and HR all speak the same language.
Template C: Modified Duty Offer Letter. A short written offer the worker signs, capturing the assigned tasks, the matching restrictions, the schedule and pay, the expected review date, and a clear statement that the assignment is temporary and transitional. A written offer protects everyone and removes ambiguity.
Template D: Ownership and Activation RACI. Who is responsible, accountable, consulted, and informed at each step?
| Step | Safety | HR | Operations | Clinical partner |
|---|---|---|---|---|
| Maintain task bank | Responsible | Consulted | Consulted | Informed |
| Confirm restrictions | Informed | Informed | Informed | Responsible |
| Make written offer | Consulted | Responsible | Consulted | Informed |
| Supervise transitional work | Informed | Informed | Responsible | Consulted |
| Track outcomes | Responsible | Consulted | Consulted | Consulted |
Where the clinical piece comes in
A modified duty library is only as good as the restrictions feeding it, and the speed at which those restrictions arrive. This is the part employers most often get stuck on, because restrictions come from clinicians, and the gap between injury and clear, current restrictions is exactly where lost time accumulates.
This is where HealthcareLive fits the framework. Our Remote Injury Care service connects an injured worker to a board-certified occupational medicine clinician within minutes, around the clock, so documented, accurate restrictions can be in a supervisor’s hands the same shift the injury occurs, not days later. For employers with on-site coverage, our On-Site Programs put an athletic trainer in the facility to evaluate, set, and update restrictions in real time. And our Virtual MSK Care keeps recovery moving with structured therapy that has helped workers return to full duty meaningfully faster, so transitional duty is a brief bridge rather than a long parking lot.
In other words, the library is your half of the system, and fast, accurate clinical restrictions are the other half. Put both together, and the activation workflow in Step 6 actually runs at the speed it needs to.
The bottom line
The difference between a modified-duty program that works and one that fails is almost never about effort in the moment. It is preparation before the moment. Reactive programs ask a stressed supervisor to invent a suitable job for an injured worker under pressure, and they lose days, claims, and people in the gap. Proactive programs do the thinking in advance: standardized restrictions, a real task bank by department, clear ownership, and a clinical partner who can deliver restrictions on the same shift.
Build the library once, keep it current, and you convert your biggest source of lost-time cost into one of your most controllable. A 40% reduction in lost-time claims is well within reach, and the research suggests the ceiling is considerably higher. If you want help connecting the clinical side of this framework to your operation, HealthcareLive can show you how it works.
Frequently asked questions
What is the difference between modified duty and transitional duty? The terms are often used interchangeably. Both refer to temporary, restricted work that lets an injured employee keep working while they recover. Many practitioners prefer “transitional duty” because it emphasizes that the arrangement is temporary and the goal is a return to the employee’s usual role, not a permanent reassignment.
Why do most modified duty programs fail? Because they are reactive. The policy exists on paper, but no specific transitional jobs have been identified in advance, so when an injury happens, a supervisor has to invent an assignment under pressure. The delay and improvisation lead to lost days, frustrated workers, and underused programs. Proactive programs that pre-build a task library by role and restriction level avoid this entirely.
Can a modified duty program really cut lost-time claims by 40%? Yes, and the published research suggests that it is conservative. Structured return-to-work programs have been documented to reduce lost workdays by as much as 55%, and one 10-year study found that lost-time claims fell by 73% and total costs fell by 54%. Results vary by employer, industry, and the rigor with which the program is run, but a 40% reduction is a realistic target for an organization that builds a genuinely proactive program.
Who should own the modified duty program? Ownership should be split clearly. Safety typically maintains the transitional task bank; HR owns compliance and the written offer process; Operations supervises the transitional workday-to-day; and a clinical partner owns the medical restrictions. Assigning these roles before an injury occurs is what keeps the program from becoming no one’s responsibility.
How fast does an injured worker need to start transitional duty? As fast as possible, ideally without losing a scheduled shift. Both the indemnity cost clock and the psychological drift toward not returning begin the moment a worker goes home. This is why immediate clinical restrictions matter so much: the sooner you have documented restrictions, the sooner you can match the worker to suitable transitional work.
Does light duty have to be meaningful work? Yes. Busywork signals to the injured worker that they are a burden and undermines the program. The most effective transitional assignments are genuinely useful tasks that a department actually needs done, which is why the “extra pair of hands” exercise with each department leader is central to the build.
Sources and methodology
External research and reporting cited in this article includes the American College of Occupational and Environmental Medicine on the decline in return-to-work likelihood with time out of work; a ten-year return-to-work outcomes study published in the Journal of Occupational and Environmental Medicine, as reported by McGriff and Sheakley, showing lost-time claims down 73% and total workers’ comp costs down 54%; ICW Group and other carrier guidance on lost-workday reductions of up to 55%; the RAND Institute for Civil Justice on reductions in missed time per claim; Bureau of Labor Statistics data on injured workers’ desire to return to work; SFM Mutual Insurance and the Amaxx Workers’ Comp blog on transitional duty design and pre-identifying transitional jobs by industry; and National Safety Council injury cost figures. Reduction ranges vary by employer, industry, claim mix, and program rigor.
Service descriptions and outcomes attributed to HealthcareLive, including Remote Injury Care, On-Site Programs, and Virtual MSK Care, reflect HealthcareLive’s own program design and network experience. The 40% lost-time claim reduction in the headline is presented as an achievable target consistent with the published ranges above, not as a guaranteed result; actual outcomes depend on how the program is built and run.



